I. General Considerations
AS stated in the Preface, there will be advanced in this work the conception of a single, 'saccharine disease', due to the consumption of refined carbohydrate foods, and with various manifestations in individual persons dependent on personal make-ups in the parts of the body affected. The conception of this disease did not dictate the evidence for it -- the evidence dictated the conception, as will be readily seen from the facts set out in the following chapters. But it is nevertheless desirable at the present moment to consider the conception from a different point of view -- the evolutionary one.
Of all the foods that exhibit an alteration from the natural state, the refined carbohydrates -- represented in this country chiefly by sugar and white flour -- exhibit the greatest. In the former approximately 90 per cent of the sugar-beet or sugar-cane has been removed, and in the latter 30 per cent of the wheat has been removed.
Furthermore, it is to be noted that these alterations are so recent by evolutionary standards of time as to date but from yesterday. It is true that, apart from earlier evidence from Egypt, white flour was being produced in Greece at least as early as 500 B.C., and Hippocrates himself recommended white bread for diarrhoea, which shows that it was already realized as passing through the gut at reduced speed. [1] Furthermore, a quotation from Antiphanes, written before 350 B.C., shows that bakers were by that time producing white loaves in quantity, and in A.D. 50 the production of white flour was geographically widespread, though socially confined to the higher grades of society in all the countries producing it. [2] In Britain, from the time of the Roman occupation, the flour was ever more frequently sieved to remove the bran, but even at the end of the sixteenth century white bread had not yet appeared in the cottages of the poor, though by the end of the seventeenth century some of the poor were eating it. However, at the end of the eighteenth century [3] practically all the poor were eating white bread, and so the turn of that century -- i.e. around the year 1800 -- is an approximate baseline, as it were, for the dating of general white flour consumption in this country.
And as regards sugar (which in this book means, unless specified as occurring in raw fruit or other natural foods, the ordinary white and brown table sugar sold in grocers' shops), Fig. 1 shows the extraordinary recentness of the alteration, in which a consumption in this country of about 15 lb. per head per year in 1815 has risen to about eight times this figure -- i.e., to about 120 lb. -- today, over 150 years later.
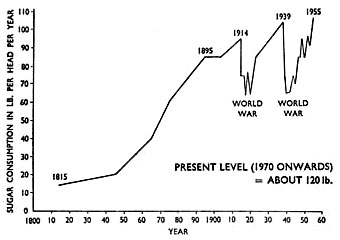
Fig. 1. -- The rise in sugar consumption in the United Kingdom over the last century and a half. (Drawn by the author from information kindly supplied by Fairrie + Co. and the 'Board of Trade Journal', and reproduced, by permission, from the 'Journal of the Royal Naval Medical Service' (1956), 42, No. 2, 55.)
|
It follows, therefore, both from the magnitude, and from the recentness, of the alterations in these refined carbohydrates, that a grievous lack of adaptation in the body to their consumption is likely to be present.
Contrast in both particulars the practice of cooking food, which not only involves a relatively trifling alteration in its constituents, but also, as regards the time factor, is of an antiquity to match the discovery of fire itself, some half a million years ago. [4] Consequently, we are now well-adapted to the practice of cooking.
As set out in an earlier work [5] referring to the saccharine disease, the refining of carbohydrates produces its very harmful results in three main ways:
- By the removal of fibre, which removal directly affects the teeth, stomach, and colon and has important repercussions on the lower venous system; such removal of fibre has formed the basis of the author's conception since it was first presented in 1956.
- By over-consumption, stemming from the concentration produced in the carbohydrates by the removal of fibre just mentioned, which over-consumption causes many serious conditions.
- By the removal of protein, which dangerously affects the behaviour of the gastric acid.
The third of these mechanisms will be discussed later, in Chapter X, on peptic ulcer, but the second mechanism, itself based on the first, calls for considerable amplification at this point. The over-consumption, as stated, stems from the concentration present in refined carbohydrates, which concentration not only deceives the taste buds in the tongue, so that they cannot signal accurately enough when to stop eating these foods, but also interferes with the normal distension of the stomach and hence with the feeling of satiety. This is all easily perceived if eating a small quantity of sugar, say roughly a teaspoonful, is contrasted with eating the same quantity of sugar in a natural form, such as exists in an ordinary apple. A person can take down teaspoonfuls of sugar fast enough, whether in tea or any other vehicle, but he will soon slow up on the equivalent number of apples. No deception takes place with these. The argument can be extended to contrasting the 5 oz. of sugar consumed, on the average, per head per day in these islands with up to a score of average-sized apples, or with a large sugar-beet weighing some 2-1/2 lb., in which this quantity of sugar approximately is present. Who would consume that quantity daily of the natural food? Or if he did, what else would he be eating? Much of the rise shown in Fig. 1 stems from this cause.
In the case of white flour the concentration that has been produced is less than in the case of sugar, and so the over-consumption that results is less, too; but that over-consumption does result can readily be seen if eating light, puffy, white bread is contrasted with eating the heavier, denser article represented by a true wholemeal bread. The fact that the rising consumption of sugar during the last century has been accompanied by a falling consumption of (predominantly white) flour does not permit the exoneration of the latter. Such alteration in consumption merely exchanges some of the damage inflicted by the flour for the still greater damage inflicted by the sugar -- and there remains the damage inflicted by the amount of white flour still being consumed.
II. The Refining of Flour and Sugar, and the Relative Dangers of the Two
1. Evolutionary Considerations
As regards which of the two refined carbohydrates, white flour (starch component of) and sugar, is the more dangerous, we must first state that the main difference between the two is a quantitative one. Qualitatively, both starch and sugar end up in the body as glucose, though we shall amplify this statement later, but quantitatively the refining processes concentrate the sugar some eight times as much as they concentrate the flour, and therefore evolutionarily the sugar emerges as much the more dangerous of the two, being that much more removed from the natural state. For it is the unnaturalness that governs the deception of the tongue and appetite, and therefore the danger of over-consumption.
2. Historical Considerations
a. The Refining of Wheat
Although white flour was being generally consumed in this country by the year 1800, as stated above, it is a fact that around the year 1880 the introduction of steel rollers into milling practices enabled a still whiter flour to be produced (70 per cent extraction instead of 80 per cent extraction). It is very important that the relative consequences of this innovation should now be assessed, for on it might be blamed the emergence of the saccharine disease. Let us therefore examine the innovation in detail.
Now it is a crucial fact that in the milling of grain the fibre (bran) is not removed evenly from the grain as the degree of milling increases. The fact is, as the author has pointed out, [6] that the fibre in grain is placed mainly on the outside of the grain, to protect it from injury, just as a hard shell protects the underlying nut. Therefore, the fibre in grain is mainly removed in the earlier, lighter degrees of milling. This is beautifully shown in Fig. 2, modified from the diagram in the book entitled Bread by Lord Horder, Sir Charles Dodds, and T. Moran, [7] which reveals that a flour containing even as much as 90 per cent of the original grain has already lost most of its fibre (bran). Indeed, the same diagram shows that the steel-roller mills of 1880 only removed an extra 9 per cent or so of the fibre already removed by the old stone-grinding mills. In the case of Canadian wheat, the figure of 9 per cent is reduced to only 6 per cent -- and twice as much Canadian wheat is used in the United Kingdom as English wheat. Meanwhile, at around the same date the consumption of refined sugar was rising by leaps and bounds, as seen on the sugar chart (Fig. 1).
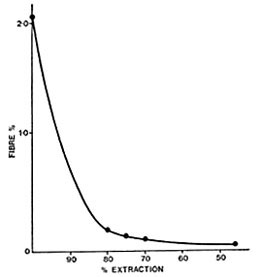
Fig. 2. -- Graph showing the smaller percentage removal of fibre with each increase in the degree of refining of flour. (Adapted by the author, with permission of the publishers, from 'Bread', by Lord Horder, Sir Charles Dodds, and T. Moran (Constable, 1954), page 54.)
|
Now since it will be shown in this book that the outbreak of the saccharine disease mainly occurred from around the year 1900 onwards, and given an incubation period, shortly to be described, ranging up to 40 years (depending on the manifestation concerned), it follows that the outbreak must mainly be ascribed to the refining of sugar, as already deduced from evolutionary considerations. And this is true whether there is concerned the manifestations of the disease due to loss of fibre directly, or those due to the loss of fibre indirectly, via over-consumption. For if the outbreak had been mainly due not to the refining of sugar but to the refining of flour, it would have occurred about a century earlier, since we have seen that by the end of the eighteenth century nearly all the population in Britain were eating white flour -- and that meant flour containing about 80 per cent of the original grain, with most of the fibre already removed.
b. The Refining of Sugar
It could still be contested, however, that although sugar consumption was rising so strongly at the above period, it was not displacing an equivalent consumption of the natural parent sugar-cane or sugar-beet. This is true, but the displacement took place by proxy. Let this be demonstrated by a few simple examples.
As the sugar gets more concentrated, so it becomes more exciting to the taste. For example, red currants on a bush are moderately attractive, but a good red-currant jelly, containing, as it does, added sugar, is much more attractive. And there lies the trouble! How can the young people of this country today, forever chewing some concentrated sweetmeat, be expected to seek out those natural analogues that, in more primitive circumstances, would be so desirable to them? Even such sweet fruits as the banana appear rather dull by comparison, and as for sweet vegetables like the parsnip -- who on earth wants to be bothered with things like parsnips any more? How many apples would be eaten at a pop festival, by comparison with ices and sweetmeats?
Nor must it be forgotten that, through the agency of evolution, the body's instinctive desires for proteins, fats, and carbohydrates, though varying in individual persons, still bear to some extent a natural ratio to each other in any one person. If, then, the desire for carbohydrates is neutralized by the taking of concentrated sweetstuffs, it will not only be sweet fruits and vegetables that undergo a fall in consumption, but also potatoes and various grains, for the starch in these eventually ends up in the body as sugar, too, and so affects instinctive carbohydrate desires. And even some refined grains, let alone the humble potato, have more fibre than refined sugar, which has no fibre at all. Hence the above argument on refined sugar versus refined flour still holds, even though it chiefly holds by proxy -- by sugar-displacement of other, less concentrated, carbohydrate foods, such as bread.
3. Considerations based on the Results of Restitution
We now come to what is considered here to be the decisive consideration in assessing the relative dangers of white-flour consumption and sugar consumption -- the results of restitution. If the experience of the present author counts for anything, who introduced the unprocessed bran into human therapeutics 40 years ago [8] and has been employing it -- often on a very large scale -- ever since, the replacement of the present white loaf in the diet of Westernized countries by the pre-1880 white loaf, both qualitatively and quantitatively, would make only a negligible difference to average intestinal transit times. People who were constipated before would remain for practical purposes just as constipated still. This he considers as certain as anything in this life can be.
But what is even more important, the introduction of a true wholemeal loaf into Westernized diets like our own, with its average sugar consumption of some 5 oz. per head per day, would by no means restore natural transit times, either. The transit times would be improved, certainly, and people who were constipated would experience some relief -- but not a decisive relief. As long as the sugar-displacement of fibre, described above, remained, no true relief would ever be obtained. To that statement, too, the author unconditionally commits himself, and he submits that were it not correct, the seven million aperient-takers in this country, to be referred to later, would long ago have switched over to wholemeal bread of themselves.
Increasing the consumption of fibre by the taking of additional bran, especially of the unprocessed type, to compensate for the fibre displaced by sugar is another matter and would certainly do the trick, as the saying is, over transit times.
* * *
But alas! this is not the end of the story. For so far we have only been discussing the direct effect of fibre on the gut, in which the fibre, or bran, derived from grain is invaluable, but when we come to discuss the indirect effect of fibre, in controlling over-consumption, the picture changes at once. This is because, though the bran would certainly correct the over-consumption from eating white flour, it would signally fail to correct the over-consumption from eating sugar -- which is far the more serious over-consumption of the two. The reason for this failure is partly because the fibre present in most fruits and sweet vegetables is much bulkier than the fibre or bran derived from grain, and therefore satisfies the appetite much more effectively; but mainly because the desire for sweetness is one of the strongest of desires where food is concerned, and unless the fibre is allied naturally to sugar, as in fruits and sweet vegetables, so that this desire for sweetness is neutralized, the correction of the over-consumption from eating sugar will seldom be achieved -- most people will just break the rules and eat sugar or foods containing sugar, such as chocolate. Anyone can take the bran and prove the foregoing for himself.
These considerations, together with the fact, as will be set out shortly, that the conditions caused by over-consumption, such as obesity, diabetes, and coronary disease, are even more serious than those arising directly from the loss of fibre itself, show very clearly that sugar is far more dangerous to the human body than is even the whitest of flour.
In order to deal successfully with over-consumption and with the dental conditions, it will be imperative not only to substitute wholemeal bread for white but also substantially to substitute natural sweet things for sugar, such as raw fruit, sweet vegetables, and certain dried fruits, like figs, raisins, and currants, as set out in the diet card at the end of this book. Trying to do without sugar often fails, but the above natural substitution for it can be very successful, and should be carried out to the limit the purse can afford. Such a procedure also usually renders superfluous the taking of any additional bran. Indeed an aphorism becomes possible here: 'In anyone taking a true wholemeal flour, the need for taking unprocessed bran as well is roughly proportional to his or her consumption of (refined) sugar.'
Finally, taking sweet-tasting chemicals like saccharin is rejected here as a solution to the problem of over-consuming sugar. Quite apart from possible dangers in the prolonged taking of this coal-tar derivative, there is also the important question of depriving the body of a class of foodstuff (sugar) which, as already said, is desired for its taste almost more than any other, and which in its natural form must therefore be of very great value. Such a step, it is submitted, would be an example of trying to be clever at Nature's expense, i.e., at the expense of evolutionary adaptation. The author, himself, would rather take a small amount of sugar. Furthermore, a low blood-sugar, i.e. hypoglycaemia, might result in faints and motor accidents in certain people.
III. A Further Note on Bread
Although the author of the present work has for many years incriminated refined sugar to a far greater extent than refined flour, as shown above, he could never agree with Professor J. Yudkin that a preference for brown (wholemeal) bread over white bread, based on nutritional grounds, is akin to 'colour prejudice'. To the author, wholemeal bread, quite apart from its crucial biochemical advantages, especially in fibre, stands for natural nutrition and for health, whereas white bread stands for unnatural nutrition and the degenerative diseases. To many peoples on this globe bread (or rice) is still the staff of life, and to these peoples the distinction between the two types of bread (or of rice) could spell the difference between life and death. But even to those peoples (and especially to those individual persons) to whom bread is not the staff of life, the difference is still one of very real importance. Furthermore, those who deliberately stick to the natural or evolutionary path over bread, and those who carelessly depart from it, are very likely indeed to do the same over other foods. The choice of bread is therefore doubly significant.
The author is well aware of the argument commonly heard, that the missing substances in white bread can always be replaced from other foods. But can they, in practice? Let us look into this assertion more closely. First of all, how many people know how to make this replacement? Second, how many people can afford to buy the necessary amounts of fruit and vegetables, where the fibre is infinitely more expensive than it is in wholemeal bread? Thirdly, in the case of old people, how many can find the energy to forage for these foods, living as they often do in some little old top room on their own? The present author stands firm on the supreme importance in personal and national nutrition of eating a true wholemeal bread. Experience has taught him how dangerous it is to try to be clever at Nature's expense, as already referred to.
IV. Statistics on Fibre-Loss
It has been argued that there has been no fall in the fibre-content of the British diet over the last 100 years, [9] and, from what the author has presented above, it is clear that most cereal fibre was lost by the year 1800, and much of the sugar-displaced fibre was lost before the year 1890, when the consumption of sugar was nearing present exalted levels. So it is true that comparatively little extra fibre has been lost over the past 100 years. (The situation in the United States would be quite different, owing to the fall in maize consumption, as set out in Chapter III. No maize is eaten in the United Kingdom.)
But this makes no difference to the conception presented in this book. For the saccharine disease has been with us on a big scale from the beginning of the present century (i.e. for the last 70 years), and some of its manifestations from long before that; furthermore, it will shortly be seen that the incubation periods of its manifestations extend in some cases up to 40 years, so that even an unchanged fibre-loss over the last 100 years, as now under discussion, would be amply accommodated by the conception.
But in truth no one, it is submitted, can really know what the fibre-loss has been over the last generation, let alone over the last 100 years. Even a generation ago allotments were common and gardens were prized; many vegetables and soft fruits were cultivated. Today allotments have largely been built over and it is easier to sell a house without a garden than with one; there is far less cultivation of vegetables and fruits. How many people go blackberrying in the countryside today compared with this common event years ago? One cannot be guided too much by Board of Trade returns; the whole tenor of our lives has altered and is still altering -- and with it has altered the personal cultivation of vegetables and fruits, for the consumption of which no statistical records can exist.
But all this is idle talk compared with the medical realities today, which comprise inter alia the present enormous sale of aperients, to some seven million people in these islands alone, as will be shown later; and the immediate relief from this state of affairs by the restitution of the fibre lost through the consumption of sugar and white flour. We are not really concerned, either here or anywhere else, with the uncertainties of the past, but with the clear indications of the present. We must judge by results, today.
V. Qualitative Considerations in the Consumption of Sugar and White Flour
The reason why little allusion has so far been made to qualitative differences, as opposed to quantitative differences, in the consumption of sugar and white flour, is that though the starch in white flour is digested to and absorbed as glucose, whereas sucrose (i.e. ordinary table sugar) is absorbed as fructose as well as glucose, these qualitative differences are natural ones and therefore have little claim on our attention compared with the highly unnatural quantitative differences so far described. In this connexion it is to be noted that many fruits abound in fructose, as the word indicates.
In amplification of the above, although the starch in flour yields glucose on digestion, whereas (table) sugar (sucrose) yields fructose as well as glucose, and although the metabolic pathway of fructose in the body is different from that of glucose, the conversion in the blood-stream of fructose into glucose (assuming the fructose is taken in natural amounts, as opposed to experimental amounts) is so rapid that this difference between glucose and fructose becomes of little practical importance. This is shown, for example, in the usual failure to substitute with advantage fructose for glucose in most clinical treatments (e.g. in diabetic coma). [10]
We therefore come back to the quantitative difference between white flour (being less refined) and (table) sugar (being more refined) already carefully discussed, and in this connexion Swan, Davidson, and Albrink [11] have shown how much faster is the digestion and absorption into the blood-stream of (table) sugar than the starch in flour (partly owing to the presence of other and impeding materials in the latter case, like the protein present in flour); and it will be seen in Chapter VII, on diabetes, that it is the speed of the glucose impact, not its size, that upsets the evolutionary adaptation in the pancreas and is held here to cause the disease. Similarly, starch and (table) sugar lead to different degrees of change in the lipids and other constituents of the blood, but these changes cannot be pursued here.
VI. The Main Manifestations of the Saccharine Disease, in Relation to the Taking of Refined Carbohydrates
We now come to what the author, after many years of thought, plus trial and error in practice, considers is the correct assignment of disease to the loss of fibre, over-consumption, and loss of protein, respectively, that were described at the beginning of this chapter as the three main consequences of the refining of carbohydrates. The grouping given is not always to be considered absolute -- for example, in the E. coli conditions the effect of over-consumption on the bacterial proliferation in the intestine is aggravated by the stasis caused by loss of fibre. Nor are all the conditions involved set down in this grouping, as will be elaborated later.
- By the removal of fibre:
a. Simple constipation (intestinal stasis), with its complications of venous ailments (varicose veins, deep venous thrombosis, haemorrhoids, and varicocele), diverticular disease, and, in part, cancer of the colon.
b. Dental caries (in conjunction with the taking of sugar) and periodontal disease.
- From over-consumption:
Diabetes.
Obesity.
Coronary thrombosis.
Primary E. coli infections and gall-stones.
- From the removal of protein:
Peptic ulceration.
The separation of the manifestations into groups in this manner is not merely a matter of convenience, but also has a direct bearing -- via clinical associations -- on aetiology and treatment. For though there is a loose clinical association between all the manifestations of the saccharine disease, the manifestations in one group (i.e., caused by one mechanism) are naturally much more closely associated with each other clinically than with those in another group (i.e., caused by another mechanism). For example, it will be shown in later chapters how closely associated with each other are the conditions due directly to loss of fibre, such as intestinal stasis, diverticular disease, haemorrhoids, and varicose veins; and in later chapters, too, how closely associated are the conditions due to over-consumption, and only indirectly to loss of fibre, like obesity, diabetes, and gall-stones.
The best paper known to the author on the latter associations (i.e., those stemming from over-consumption) is that by M. D. Kaye and F. Kern. [12] Even these iconoclasts admit a probable clinical association between obesity, diabetes, and gall-stones. The author himself, and others whose studies have been widely reported, would put it much more strongly than that; and he would also add coronary disease to this group, which Kaye and Kern also propose should be added, but the association of which they do not regard as proved. However, at least the crucial association of coronary disease with diabetes now appears to be very generally accepted, and will be elaborated on later in this work.
These clinical associations clearly throw much light on aetiology. [13] For example, it will be shown in Chapter VIII, on coronary disease, that with the close association between this disease and diabetes, and with the strongest reasons for believing diabetes to be caused by over-consumption from the taking of refined carbohydrates, and only indirectly caused by the loss of fibre in these carbohydrates, it is reasonable to consider the same cause for coronary disease itself.
But the separation of the manifestations into the groups set out above bears directly on treatment, too. [13] For the adding of unprocessed bran to the diet, as described earlier (and later), will have a magical effect on conditions like constipation, haemorrhoids, and diverticular disease, but little or no effect on obesity and diabetes. For the first group, being due directly to loss of fibre, is alleviated by the restitution of any type of fibre; but the second group, being due to over-consumption and only indirectly to loss of fibre, is alleviated by the restitution of fibre only to the extent that this corrects over-consumption, not only of flour but also of sugar, as already explained.
Thus, in the writer's opinion, it would be as futile to try to arrest coronary disease with bran as it would be to try to arrest latent or early diabetes with bran (or, for rather different reasons, to arrest dental decay and periodontal disease). A type of fibre restitution which also corrects sugar consumption is absolutely essential in conditions like these, and bran supplies neither the bulk nor the natural amount of sugar needed for success. The type of restitution needed is, indeed, set out in the natural-diet card at the end of this work, as already stated.
It may be added here that the importance of over-consumption (especially of sugar), as distinct from direct loss of fibre, in the production of many manifestations of the saccharine disease, is well seen in the explosive outbreak of this disease now taking place in the Canadian Eskimoes, following on their sugar consumption passing 100 lb. per head per year. This has recently been set out in a comprehensive manner, [14] and it will be seen later that dental caries, appendicitis, diabetes, and gall-stones are now rampant amongst these people, and in the author's opinion other manifestations (especially coronary disease) will certainly follow. But it is impossible to explain these events by much loss of fibre. For the natural diet of these Eskimoes has always been conspicuously lacking in fibre, which has seldom exceeded the fibre found in the faeces of the reindeer, sometimes eaten by them as a vegetable during the summer months, and the fibre found in bilberries, also eaten at that period. (In the natural Eskimo diet the chewing of raw meat replaced the effects of fibre on the teeth and gums, and the eating of seal fat largely replaced the aperient effects of fibre on the intestines; for practical purposes no sugar was eaten.)
In fact, the Eskimoes pursuing a sophisticated existence today consume far more fibre -- from the eating of tinned fruits and certain vegetables -- than ever they did in their natural existence. Yet, as said, many manifestations of the saccharine disease are now becoming common to them, which shows the much greater importance of over-consumption in the production of many saccharine manifestations. And since sugar is by far the most refined carbohydrate, it is in sugar that this over-consumption is always most conspicuous and most in need of correction. And the same applies, though in a slightly different manner, in dental decay and periodontal disease.
VII. The Question of Proteins and Fats
To turn now to the other two main classes of food, whilst proteins are rarely appreciably altered from the natural state, it is true that some fats, such as butter and certain vegetable oils, show a very large alteration, and indeed a concentration comparable to that produced in the refined carbohydrates. But the concentration here never seems to deceive either the tongue or the appetite, and the reason for this, in the author's opinion, is that fat in Nature often occurs in pure form, such as the fat in meat. For instance, butter and margarine contain about 85 per cent fat, whereas, to give an example of the fat in meat, the perinephric fat (suet) in oxen and sheep contains about 99 per cent fat. The result is that the tongue and the appetite are evolved to cope with the consumption of pure fat and no over-consumption occurs. Thus, no more fat would be consumed in the case of bread and butter or bread and margarine, where the fats have been concentrated artificially, than in the case of bread and dripping, where the fat is equivalent to the pure fat in beef, that can be cut off with a knife and shows no concentration at all. Certainly a person's tongue is a very sensitive guide indeed to his fat requirements, whatever type of fat is involved. Some people are Jack Sprats, who can eat no fat, and some are the opposite. In close accord with all this, the rise in fat consumption per head in the Westernized nations over the last century or so has probably been only about 25-50 per cent. [15, 16] Indeed, M. A. Antar and others have recently shown that total fat consumption in the United States has increased by only 12 per cent over the last 70 years, [17] and similar figures have been collected by B. Friend. [18]
To sum up, then, there is no doubt, from an evolutionary point of view, that, in any disease in man due to alterations in his food from the natural state, the refined carbohydrates, both on account of the magnitude and the recentness of the alterations, are always the foods most likely to be at fault, and not the fats. It will be seen in the following chapters that the incrimination of the refined carbohydrates on evolutionary grounds is supported by equal incrimination on epidemiological grounds, and the conception of a single saccharine disease is thus based on two independent foundations.
VIII. Harmlessness of Unrefined Carbohydrates
The conception set out above, of mankind not being adapted to the consumption of refined carbohydrates, must be carefully distinguished from that advanced by J. Yudkin, [19] that the human body is not properly adapted to the consumption of unrefined (i.e. natural) carbohydrates either, because 'with the discovery of cereals some ten thousand years ago, man for the first time became a food producer and ceased to rely on gathering and hunting his foods'.
The present author cannot accept this view, for three separate reasons.
Firstly, he does not hold that man until ten thousand years ago was primarily a carnivore. To quote from H. M. Sinclair's [20] objection to the same view: 'When man first started to keep his forepaws off the ground he ate fruit, nuts, and berries, as do the apes to-day; he could not kill and eat woolly rhinoceroses without fangs or claws. When he had tools he hunted and ate animals, including himself, but in the Chellean and Acheulian epochs he was probably vegetarian, apart from gathering grubs.' However, exactly what man ate in bygone ages must be largely conjectural; what is not conjectural is the structure of the human body today, which indicates with much clarity that man is further from being a pure carnivore than from being a pure herbivore. Though in fact omnivorous, he is, as Sinclair states, most typically a frugivore or fruit-eater -- which is much closer to the herbivore than the carnivore. Thus man lacks the carnassial teeth for tearing flesh, and the rasping tongue of the carnivore (though he also lacks the specialized molars of the herbivore). His saliva contains the ferment, ptyalin, for digesting starch, characteristic of the herbivore, whilst his gastric juice, also like that of the herbivore, contains only a fraction of the hydrochloric acid present in the carnivore. There is not the least doubt that man is fully equipped to live on plant foods, as indeed many hundreds of millions of rice-eaters in China, India, and elsewhere abundantly reveal today.
Secondly, Yudkin's conception implies that man cannot rely on his sense of taste when eating foods in their natural state -- i.e., that his sense of taste may be evolved out of harmony with the rest of his body, so that he may like eating whole cereals or other natural carbohydrates without being able properly to metabolize them. But logic dictates that the body is evolved harmoniously, as a whole; and so does the evidence, too, for a herbivore, like a horse, will die of starvation rather than eat meat or other animal foods, which it cannot metabolize; whilst a carnivore, like a lion, will die of starvation, too, rather than eat grass or other plant foods, which it likewise cannot metabolize.
Thirdly, and most important of all, it will be the endeavour of this work to show that all the manifestations of the saccharine disease discussed are strikingly absent in those races still subsisting almost exclusively on just these unrefined carbohydrates.
In this connexion it is to be noted that the occurrence of diseases like kwashiorkor, common in eaters of grain, like maize, even when eaten unrefined, in no sense indicates any lack of adaptation in the body to the consumption of these grains. The truth is that man cannot live exclusively on any one type of foodstuff, and if he tries to do so, he suffers from a deficiency of the other types. Kwashiorkor occurs in those who live on maize and other grains -- but on practically nothing else. It is a deficiency disease, and it would be as illogical to relate it to lack of adaptation to these grains as it would be to relate scurvy, occurring on a pure meat diet, to lack of adaptation to meat. And as regards the rare cases of allergy to (usually recently introduced) carbohydrate foods, it is submitted that these would be still rarer in the absence of the arbitrary food mixtures described in Chapter X.
It is considered, then, that unrefined carbohydrates, including the starch in cereals and tubers, and the sugar in fruit, sugar-beet, and sugar-cane, are absolutely safe to eat in their natural state, and that trouble only arises when they are eaten after being refined from that state. One or two small exceptions are discussed in Chapter X.
The distinction between these two views is fundamental, and has a direct bearing on treatment, as will be seen in all the conditions (including even obesity) to be discussed in this work, where the aim will always be to eliminate the refined carbohydrates, never the unrefined, natural carbohydrates.
IX. Incubation Periods in the Saccharine Disease
It is important to remember that it takes time for the consumption of refined carbohydrates to produce the various manifestations of the saccharine disease. In short, these manifestations have incubation periods, which differ in each case. In some manifestations the incubation period is very short. Thus, a massive dose of sugary material could cause so great a proliferation of intestinal organisms that in some E. coli conditions, such as appendicitis (especially in children), the incubation period could be a matter of hours, and it will be seen later that sweetened dummies can cause the destruction of all the milk teeth from decay in a matter of months. But it will also be seen that in the case of diabetes the incubation period may be 20 years, in the case of coronary disease 30 years, and in the case of diverticular disease 40 years.
It is clear that the incubation periods of the various manifestations will depend partly on the degree of concentration (refinement) present in the carbohydrates consumed (sugar, for example, being considerably more concentrated than white flour, which, as will be shown later, makes it especially important in the causation of E. coli conditions, like appendicitis); partly on the amounts of such carbohydrates being consumed, and partly on different personal make-ups in different persons and even in different races.
It is also clear that the incubation periods in single persons may differ from those in whole communities or whole countries. Thus, if in a country the large-scale refining of flour long precedes that of sugar, then conditions that can follow the refining of flour, such as haemorrhoids, may well precede those more intimately related to the consumption of sugar, such as the appendicitis just referred to, even though the personal incubation periods are the other way round. When evaluating, therefore, the epidemiological evidence for or against any given medical condition being a manifestation of the saccharine disease, it is clearly most necessary to look into the various aspects of the incubation period, especially in conditions like coronary disease, where the period can be a very long one.
It is clear that the long incubation period in most saccharine manifestations can render present personal appearances very deceptive. Thus, as regards R. A. McCance's and E. M. Widdowson's [21] well-known trial with German schoolchildren after the last war, one group fed on wholemeal bread and another on white bread and with both groups apparently in much the same state of health at the end of a year, these two groups could well have had very differing medical futures if they had carried on with their two different breads in later years.
To take, perhaps, the least serious example, would a bigger proportion of the white-bread children have eventually joined the great army of aperient-takers today? To judge by the present rapid spread in Great Britain of the taking of unprocessed bran for constipation, this could well have proved to be the case. And the pathway of intestinal stasis is littered with conditions like haemorrhoids, in the earlier stages of the pathway, and like diverticular disease, in the later stages of the pathway.
And as regards over-consumption, would a bigger proportion of the white-bread children have eventually joined another great army of people -- those who are over-weight? To judge by the admitted importance of very small amounts of over-consumption, if repeated day after day, year in and year out, this could well have proved to be the case too. And the pathway of obesity is littered, as we have seen, with even more serious conditions than is the pathway of stasis.
And what about peptic ulcer? When one remembers the ulcer belt of India, in which the population takes milled white rice instead of home-pounded brown rice, as will be seen in a later chapter, can it be excluded that, in spite of the greater diversity of food over here, a bigger proportion of the white-bread children would not have ended up with this complaint also?
X. Final Considerations
With regard to the groups of conditions advanced above as due to the consumption of refined carbohydrates, and together comprising a single saccharine disease, it is considered here that when any one of these conditions occurs without apparent reason, i.e., idiopathically, as is normally the case, there is no other basic cause for it than the consumption of these unnatural foods, though other, modifying factors may well be present. Far from it being difficult to believe that there is but a single basic cause for any of these conditions, it is suggested that what would be difficult to believe would be the exact opposite -- that there were multiple basic causes for it. In fact, in the author's opinion, when such multiplicity of causes is advanced, the less likely are any of them to include the right one. It is noteworthy, for example, how, by increasingly general consent, the primary cause of dental caries has gradually been narrowed down to the single one given here, and he is confident that in due course the same sequence will take place with the other conditions listed.
Nor does he consider it an improbability that the same primary cause should exist for many separate conditions, and that such attribution shows loss of perspective. On the contrary, he holds the very opposite to be the case -- that it would be an extraordinary coincidence if these refined carbohydrates, which are known to wreak such havoc on the teeth, did not also have profound repercussions on other parts of the alimentary canal during their passage along it, and on other parts of the body after absorption from the canal.
Indeed, just in the way that, as the knowledge of syphilis widened, conditions such as aneurysm of the aorta and general paralysis of the insane, which originally were never imagined as connected with the disease, gradually became added to ft as systemic manifestations, so, as the author advanced in the joint work in 1966, may this be true of the saccharine disease, which logically should involve many systems, too.
For it is much more logical that a single cause, the consumption of refined carbohydrates, like the single cause of arsenic poisoning, for example, should be regarded as resulting in a single disease with many systemic manifestations than in a whole lot of separate diseases.
Distant Horizons
The above approach points to possible new advances in the understanding of causation, and also in treatment. Thus, thyrotoxicosis appears to be a very possible saccharine manifestation. It is known to be rare in tribal Africans, but seems to be getting commoner in certain urban areas, such as Nairobi. [22] This is the classic march, both temporal and geographical, of a saccharine condition, as Western foods are introduced into primitive communities. The clue could be worth pursuing, as it would explain why, in the author's experience, the natural, unconcentrated diet appears to be beneficial in early cases of thyrotoxicosis.
Similarly, there are certain aspects of disseminated sclerosis, involving sugar consumption, [23] that suggest it may be a saccharine manifestation in the central nervous system, but these aspects cannot be pursued here. Likewise schizophrenia might represent a different type of involvement of the central nervous system, affecting the mind. The author can well imagine some astonishment on the face of the reader, but he would like to quote a personal communication from Dr. G. Daynes, of the Transkei region of South Africa, dated September, 1971: 'Regarding mental disease in the people of the Transkei, I can say that in the past 11 years I have not diagnosed a single case of schizophrenia in a tribal African living on an unrefined carbohydrate diet, whereas this disease is the commonest psychosis among the urbanized Africans. The "School people", who come in between the tribal and the urbanized, have an appreciable incidence of the disease, but they consume considerable quantities of white sugar and refined maize-meal, leading to a high incidence of obesity and a small but increasing incidence of diabetes.' It may be added to this that schizophrenia in the U. S. Negro is as common as in the white. [24] Meanwhile, the profound stasis in the bowel so notorious in cases of melancholia lends some credence to the possibility that schizophrenia may be implicated in the saccharine disease, too.
What would be the mechanism of production in the speculative manifestations suggested above, if they proved eventually to be realities? The author believes it could lie in each case in the absorption of toxins from the intestines. Indeed, he finds himself gravitating more and more to Ehrlich's conception of an intestinal toxaemia, referred to in Chapter IX, with the toxins, however, never forming as Ehrlich thought they did, under natural conditions, but only as the result of over-consumption through the taking of refined carbohydrates, and the bacterial putrefaction to which this leads (Chapter IX). The author might add that his gravitation to a modified Ehrlich conception, given above, stemmed partly from logic and partly from clinical experience in treatment.
Such toxins in the intestine could also have local implications in the causation of Crohn's disease and ulcerative colitis, which on temporal and on geographical grounds appear to have a very good chance indeed of being saccharine manifestations. [25]
One thing is very clear: in any degenerative condition of unknown causation, the adoption of the natural, unconcentrated diet appears to be strongly indicated on general principles.
The author has sometimes been blamed by his friends for resisting modifications in his conception. The reason for this does not lie, he hopes, in his getting older these days, but in the fact that he applied the conception in practice, not only widely in temperate and tropical climates but also for some 20 years as a physician in naval hospitals, before publishing anything. Therefore, with this prolonged clinical testing behind him, though the author believes that extensions to the saccharine disease will be made in the future, he does not believe that any appreciable modification of the present outline of the disease will be able to be sustained against it. He attaches great importance to the diet card presented at the end of book and the simple mechanisms behind it.
We now turn our attention away from all speculative manifestations of the saccharine disease and direct it to those manifestations about which the author believes there is no doubt whatsoever.
References
1. McCance, R. A., and Widdowson, E. M. (1956), Breads, White and Brown, 9. London: Pitman Medical.
2. Ibid., 6.
3. Ibid., 46.
4. Clarke, W. E. Le Gros (1950), History of the Primates, 2nd ed. London: Trustees of the British Museum.
5. Cleave, T. L. (1962), Peptic Ulcer. Bristol: Wright.
6. -- (1972), Brit. Med. J., 2, 409
7. Horder, Lord, Dodds, Sir Charles, and Moran, T. (1954), Bread. London: Constable.
8. Cleave, T. L. (1941), Brit. Med. J., 1, 461.
9. Robertson, Jean (1972), Nature, Lond., 238, 291.
10. Woods, H. F., and Alberti, K. G. M. M. (1972), Lancet, 2, 1354.
11. Swan, D. C., Davidson, P., and Albrink, M. J. (1966), Ibid., 1, 60.
12. Kaye, M. D., and Kern, F. (1971), Ibid., 1, 1228.
13. Cleave, T. L. (1972), Brit. Med. J., 1, 678.
14. Shaefer, O. (1971), Nutrition Today, 6, No. 6, 8; and personal communications.
15. Stone, R. (1934), Measurement of Consumers' Expenditure and Behaviour in the U.K. 1920-1938. London: Cambridge University Press.
16. Keys, A. (1953), J. Mt Sinai Hosp., 20, 119.
17. Antar, M. A., Ohlson, M. A., and Hodges, R. E. (1964), Am. J. Clin. Nutr., 14, 169.
18. Friend, B. (1967), Ibid., 20, 907.
19. Yudkin, J. (1963), Lancet, 1, 1335.
20. Sinclair, H. M. (1963), Ibid., 2, 43.
21. McCance, R. A., and Widdowson, E. M. (1954), Medical Research Council Report, 287.
22. McGill, P. E. (1971), Brit. Med. J., 2, 679.
23. Roberts, H. J. (1966), Lancet, 4, 745.
24. From information kindly supplied for the author by Charles V. Menendez, Charity Hospital, New Orleans, October 1971.
25. Leader, Lancet (1972), 2, 942.
Next chapter
Table of Contents
Back to the Small Farms Library Index

Community development | Rural development
City farms | Organic gardening | Composting | Small farms | Biofuel | Solar box cookers
Trees, soil and water | Seeds of the world | Appropriate technology | Project vehicles
Home | What people are saying about us | About Handmade Projects
Projects | Internet | Schools projects | Sitemap | Site Search | Donations | Contact us